Angioplasty and stent - heart - discharge
Drug-eluting stents - discharge; PCI - discharge; Percutaneous coronary intervention - discharge; Balloon angioplasty - discharge; Coronary angioplasty - discharge; Coronary artery angioplasty - discharge; Cardiac angioplasty - discharge; PTCA - discharge; Percutaneous transluminal coronary angioplasty - discharge; Heart artery dilatation - discharge; Angina angioplasty - discharge; Heart attack angioplasty - discharge; CAD angioplasty - dischargeDrug-eluting stents - discharge; PCI - discharge; Percutaneous coronary intervention - discharge; Balloon angioplasty - discharge; Coronary angioplasty - discharge; Coronary artery angioplasty - discharge; Cardiac angioplasty - discharge; PTCA - discharge; Percutaneous transluminal coronary angioplasty - discharge; Heart artery dilatation -...
The Basics
Tests for coronary artery blockage
A Closer Look
Directional coronary atherectomy (DCA) - Animation
Directional coronary atherectomy (DCA)
Animation
Percutaneous transluminal coronary angioplasty (PTCA) - Animation
Percutaneous transluminal coronary angioplasty (PTCA)
Animation
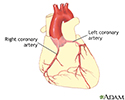
Coronary artery blockage
Atherosclerosis is a common disorder of the arteries. Fat, cholesterol, and other substances collect in the walls of arteries. Larger accumulations are called atheromas or plaque and can damage artery walls and block blood flow. Severely restricted blood flow in the heart muscle leads to symptoms such as chest pain.
Coronary artery blockage
illustration
Coronary artery balloon angioplasty - series
Presentation
Heart bypass surgery - series
Presentation


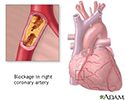

. The small arteries of the heart muscle (the coronary arteries) can be narrowed or blocked by this accumulation. If the narrowing is small, percutaneous transluminal coronary angioplasty, or PTCA for short, may be the course for treatment. PCTA is a minimally invasive procedure to open up blocked coronary arteries, allowing blood to circulate unobstructed to the heart muscle. The indications for PCTA are persistent chest pain (angina), and blockage of only one or two coronary arteries.</p>")
, a catheter is inserted into an artery at the top of the leg (the femoral artery). The procedure begins with the doctor injecting some local anesthesia into the groin area and putting a needle into the femoral artery (the blood vessel that runs from the heart down the leg). Once the needle is inserted, a guide wire is placed through the needle, into the blood vessel. Following this step, the guide wire is left in the blood vessel and the needle is removed. A large needle called an introducer is then placed over the guide wire and the guide wire is removed. </p>")
 guidewire, into the blood vessel. This catheter is then guided to the aorta and the guidewire is removed. Once the catheter is placed in the opening or ostium of one of the coronary arteries, the doctor injects dye and takes a series of X-rays (film of the images). </p>")


 are taken to check for any change in the arteries. Following this, the catheter is removed and the procedure is completed. </p>")
 may be recommended.</p>")
 sandbag may be placed over the femoral artery puncture site in the leg and remain there for 6 hours. This is done to help the artery heal. </p>")


 or heart bypass surgery is recommended when one or more coronary arteries are seriously blocked and blood supply to the heart muscle is insufficient. Several tests are done to identify the cause of the chest pain (angina), such as blood tests and x-ray studies (angiograms).</p>")

. It is done through an opening through the breast bone. While one surgeon is working on the chest, another surgeon works on taking a length of vein (saphenous vein) for the bypass through a long incision along the inside of the lower leg. The vein is sewn in above and below the blockage in the coronary artery. Alternatively, an artery from the interior aspect of the chest wall (internal mammary artery), or the arm (radial artery) is used.</p>")

. Chest tubes will be in place for the first 2 to 3 days to drain any residual blood and fluid from around the heart. Heart functions will be monitored. The full benefits from the operation may not be ascertained until 3 to 6 months after surgery. Sexual activity may be resumed 3 to 4 weeks after surgery. All activities that do not cause fatigue are permitted, but the patient must not strain the healing chest bone (sternum).</p>")
Directional coronary atherectomy (DCA) - Animation
Directional coronary atherectomy (DCA)
Animation
Percutaneous transluminal coronary angioplasty (PTCA) - Animation
Percutaneous transluminal coronary angioplasty (PTCA)
Animation
Coronary artery blockage
Atherosclerosis is a common disorder of the arteries. Fat, cholesterol, and other substances collect in the walls of arteries. Larger accumulations are called atheromas or plaque and can damage artery walls and block blood flow. Severely restricted blood flow in the heart muscle leads to symptoms such as chest pain.
Coronary artery blockage
illustration
Coronary artery balloon angioplasty - series
Presentation
Heart bypass surgery - series
Presentation
Angioplasty and stent - heart - discharge
Drug-eluting stents - discharge; PCI - discharge; Percutaneous coronary intervention - discharge; Balloon angioplasty - discharge; Coronary angioplasty - discharge; Coronary artery angioplasty - discharge; Cardiac angioplasty - discharge; PTCA - discharge; Percutaneous transluminal coronary angioplasty - discharge; Heart artery dilatation - discharge; Angina angioplasty - discharge; Heart attack angioplasty - discharge; CAD angioplasty - dischargeDrug-eluting stents - discharge; PCI - discharge; Percutaneous coronary intervention - discharge; Balloon angioplasty - discharge; Coronary angioplasty - discharge; Coronary artery angioplasty - discharge; Cardiac angioplasty - discharge; PTCA - discharge; Percutaneous transluminal coronary angioplasty - discharge; Heart artery dilatation -...
The Basics
Tests for coronary artery blockage
A Closer Look
Angioplasty and stent - heart - discharge
Drug-eluting stents - discharge; PCI - discharge; Percutaneous coronary intervention - discharge; Balloon angioplasty - discharge; Coronary angioplasty - discharge; Coronary artery angioplasty - discharge; Cardiac angioplasty - discharge; PTCA - discharge; Percutaneous transluminal coronary angioplasty - discharge; Heart artery dilatation - discharge; Angina angioplasty - discharge; Heart attack angioplasty - discharge; CAD angioplasty - dischargeDrug-eluting stents - discharge; PCI - discharge; Percutaneous coronary intervention - discharge; Balloon angioplasty - discharge; Coronary angioplasty - discharge; Coronary artery angioplasty - discharge; Cardiac angioplasty - discharge; PTCA - discharge; Percutaneous transluminal coronary angioplasty - discharge; Heart artery dilatation -...
The Basics
Tests for coronary artery blockage
A Closer Look
Review Date: 8/16/2022
Reviewed By: Michael A. Chen, MD, PhD, Associate Professor of Medicine, Division of Cardiology, Harborview Medical Center, University of Washington Medical School, Seattle, WA. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team.
 All rights reserved.
All rights reserved.